Pressure building in the chest (tension physiology)
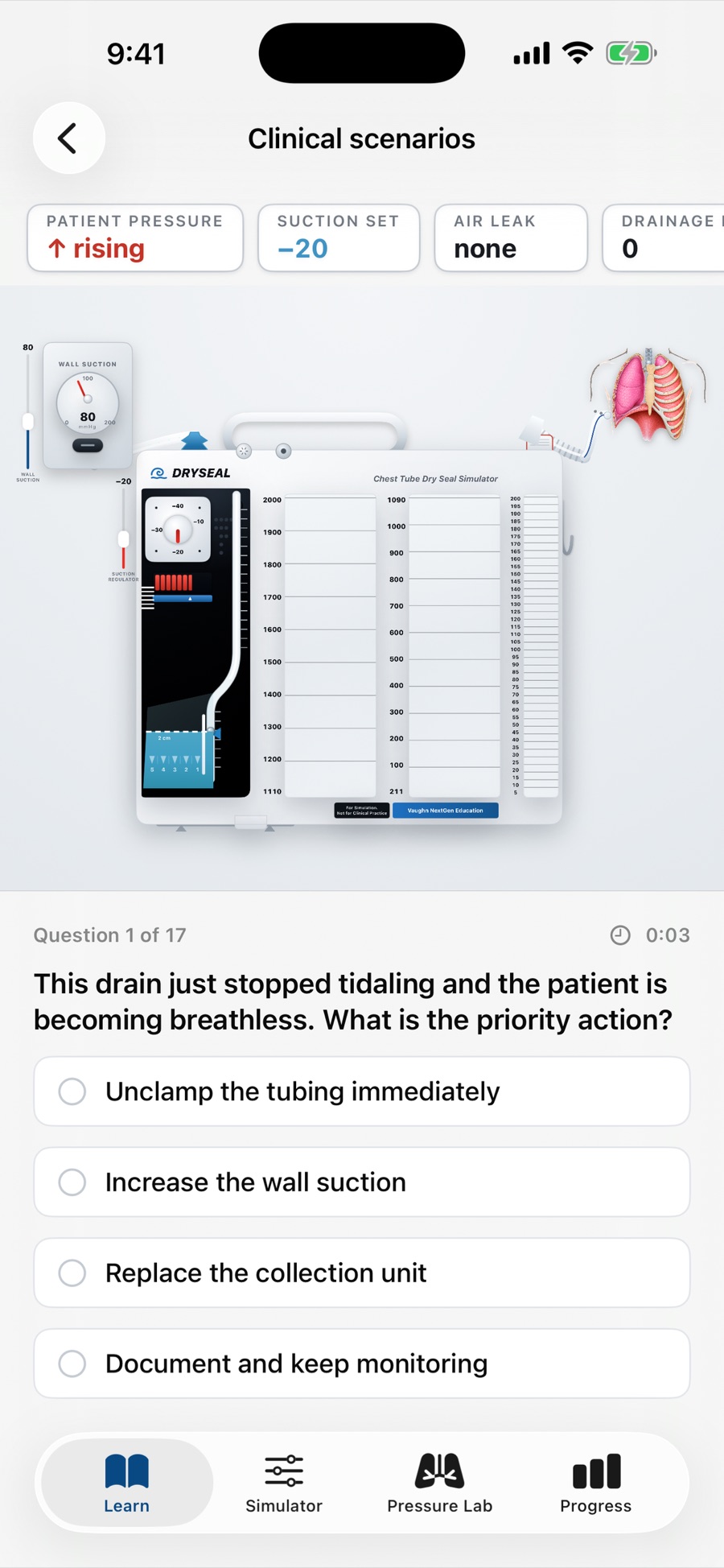
In a tension pneumothorax, air enters the pleural space and can't get back out, so pressure climbs with each breath. The picture to recognize: a patient getting more breathless and unstable — sometimes alongside a drain that has stopped tidaling or a system that isn't venting. This is a recognize-and-escalate-now situation: call for help and follow your facility's emergency protocol. Losing tidaling on its own isn't an emergency; losing it in a patient who is decompensating is.
Why routine clamping is risky
Clamping a chest tube can turn a leak into a trap — if air is still leaving the chest and you clamp it off, pressure can build. Because of that, routine clamping is discouraged. Tubes are generally only clamped briefly and for specific reasons (changing the drainage unit, momentarily locating a leak, or a physician-ordered trial before removal) — and not during transport. If a patient needs to move, the usual teaching is to keep the unit upright and below the chest so it keeps working on the water seal, rather than clamping. Always follow your unit's policy and the order.
A tube that comes out or disconnects
Two different problems, both taught as act-fast situations:
- Tube dislodged from the patient — the insertion site is now open. Get help immediately and cover the site as your facility's policy directs. Many policies use an occlusive dressing, but practice varies — a fully sealed dressing over an ongoing air leak can let pressure build, so some facilities dress it differently. This is a know-your-protocol-in-advance situation, not a one-size-fits-all step.
- Tube disconnected from the drainage unit — the sterile system is broken. Facilities teach a specific recovery step (often placing the end in sterile water to re-establish a seal) — follow yours.
Know your facility's exact protocol before it happens; that's what this kind of practice is for.
Overfilling and brisk bleeding
Watch the collection chamber. A unit filling toward its capacity needs to be addressed per policy before it overflows. A sudden increase in bright-red drainage, or a large volume in a short time, is a cue to escalate — those numbers matter, and they're worth reporting early rather than late.
Practice spotting danger in the app
Chest Tube Simulator lets you switch on the dangerous states — tension physiology, a clamped tube, overfill, a large air leak — and see how the device and the alerts respond, plus a Managing Complications quiz (one of four in the app) to test whether you'd catch them. It's a safe place to build the reflex; the real decisions still belong to you, your team, and your protocols.
FAQ
-
When should a chest tube be clamped?
Only when ordered and permitted — briefly, for specific reasons like changing the unit, locating a leak, or a removal trial. Routine clamping is discouraged, and tubes aren't clamped for transport, because pressure can build if air can't escape.
-
What do I do if a chest tube gets dislodged?
Treat it as urgent: get help right away and manage the open site per your facility's policy. Facilities differ on how to dress a dislodged chest-tube site, so learn your unit's exact protocol before it happens rather than assuming a single "right" dressing.
-
How is a tension pneumothorax recognized around a chest tube?
A patient getting more breathless and unstable while pressure builds in the chest — sometimes with loss of tidaling or a system that isn't venting. Escalate immediately and follow your emergency protocol.
-
Can I use this app to make patient decisions?
No. It's for learning and practice only — not a medical device and not medical advice. Real decisions follow your assessment, your provider's orders, and your facility's policy.